Hip dysplasia breeding schemes and PennHIP
Mike
Guilliard MA VetMB CertSAO MRCVS
Nantwich Veterinary Hospital (UK)
PRINT HERE
Canine hip dysplasia (CHD) is a common cause of pelvic limb lameness and exercise intolerance. The dictionary definition of dysplasia is abnormal growth or development and as such CHD is a developmental condition and is not congenital. CHD is prevalent in almost all breeds and must be seen as a result of breeding programmes selected to accentuate characteristics that are desirable for the various breed standards. Breeds such as the racing Greyhound, where the selection process is towards racing performance, have normal hips and do not develop the osteoarthritis (OA) of CHD.
It has long since been known that CHD is an inherited condition and as such, by identifying the carriers, it should be possible to decrease its prevalence and severity. As the condition is polygenic screening for specific genes is not yet a possibility and so identification of carriers is by phenotype and not genotype. Basically all hip improvement schemes attempt to predict the likelihood of the development of hip OA. The standard British Veterinary Association/Kennel Club (BVA/KC) hip scheme selects as its phenotype, changes to the hip joints as seen on a hip-extended radiograph with various changes to the joint being scored as to their severity. These changes fall into three categories that are basically subluxation, joint remodelling and osteoarthritis. Similar schemes include the OFA scheme of the USA, the FCI scheme of Europe and the German SV a stamp scheme.
The BVA/KC hip scheme advises owners to breed from dogs that are well below the breed mean score. However it is apparent to breeders and veterinarians that the hip status of the national canine population has not seemingly improved over the many years of the scheme’s existence. The BVA/KC will argue that breed mean standards have improved but as there is no compulsion to submit all radiographs many with high scores are not submitted saving the owner the submission fee however, skewing the breed mean scores, making them non representative.
Of the nine parameters scored on each hip by the BVA/KC, it is only the Norberg angle that can be measured objectively where as the rest are subjective assessments with both intra and inter assessor agreement variance. The scores for subluxation are also affected by positioning with the hip-extended view artificially tightening the hip joints. In addition, although OA changes are scored, no indication of its significance is given to the breeder.
The diagnostic test of any scheme has to evaluate hip phenotype as an estimate of the genotype, and its relationship is the concept of heritability. A high heritability approaching 1, means that the phenotype accurately reflects the genotype. Heritability of a given trait is lowered if environmental factors, such as diet or exercise can influence the trait’s expression. Diagnostic error also lowers the estimate of heritability making the measure less useful as a hip screening tool.
Improvements in the hip status of the offspring are also governed by the selection pressure and this is defined as the deviation of the parental mean from the population mean. An example would be breeding parents with a mean hip score of say 5 when the breed mean is 18. This would greatly increase the selection pressure whereas if the mean parental hip score was 14 then the selection pressure would be low.
As heritability is a quantitative trait it is possible to calculate the expected change in average litter phenotype after one generation using the mathematical formula, “genetic change per generation equals heritability multiplied by the selection pressure”. Conversely by knowing the hip scores of the litter it is then possible to calculate the heritability of the diagnostic test (4).
In two well-executed studies of subjective hip scoring using the OFA method in the German shepherd dog, breed estimates of heritability were 0.22 (1) and 0.43 (2), and in four other breeds it was found to be 0.26 (3). These degrees of heritability are considered low meaning that genetic change will be slow. Moreover if selective breeding does improve the hip status over a few generations then there would be a decrease in the phenotypic and genotypic variance to a point when further improvement is not possible.
This may well be contributing to the failure of the BVA/KC scheme as a steady state has been reached by the determined breeders and further improvement is not possible.
An improvement in decreasing the incidence of CHD can therefore be achieved by using a screening test with a higher heritability and ample range in the metric to enable applying significant selection pressure. The only such test available is the Pennsylvania Hip Improvement Program (PennHIP). It is the only hip screening method capable of quantifying the risk for osteoarthritis as a result of hip dysplasia, and is based on the measurement of hip joint laxity. The screening test necessitates taking three different hip views. A standard hip-extended view allows the reporting of OA already present while the compression (figure 1) and distraction (figure 2) views enable the calculation of the distraction index (DI). As the dog is anaesthetised the DI is a measure of passive hip laxity with the muscular forces on the joint eliminated.
The DI is a linear scale that directly measures the degree of hip subluxation or laxity; a DI of 0.8 would indicated that 80% of the femoral head was subluxated from the acetabulum where as a DI of 0.25 indicates that there is only 25% subluxation and thus the hips are described as tighter. There is a degree of passive joint laxity in the hips of all breeds and a DI of > or = 0.3 is considered normal with virtually no risk of developing subsequent OA. However the laxity profiles of different breeds vary as can be seen in figure 3 that plots the probability of developing OA at 24 months of age against the DI (5).
Heritability of DI varies from different studies and averages out at around 0.65 (0.42 to 0.92) but is always considerably higher than the heritability of subjective hip scoring methods. Using high selection pressure from the DI profile of the breed or of the closed colony enables rapid improvement in hip status of the offspring in just a few generations. Breeders like to select other genetic factors in breeding programmes and dogs having the tightest hips may be undesirable for other traits, but by using the DI method, providing that the breeding stock is from the tighter side of the breed mean, hip improvement can still be achieved, albeit more slowly, than if maximum selection pressure were applied.
Another huge advantage of the PennHIP method is that pups can be accurately assessed from 16 weeks of age and subsequent submissions are allowed and indeed encouraged. In addition all cases have to be submitted for analysis and therefore the breed mean DI scores are free of selection bias and more accurate.
The disadvantage of the PennHIP method is that until now it has relied on manual holding to obtain the compression and distraction radiographs and that contravenes UK radiation safety rules. However a hands-free technique has recently been evaluated that is both cheap and simple, and this will allow UK veterinarians to take PennHIP radiographs and to become PennHIP certified.
The major disadvantage of the BVA/KC scheme is that it can produce false negative results in that many dogs scored as having good hips will have an unacceptable degree of laxity and will go on to develop OA and therefore should not be used for breeding. However the strength of the BVA/KC scheme is that any dog with a high hip score will have bad hips meaning no false positives.
The PennHIP system is rapidly gaining worldwide acceptance and with more than 80,000 dogs on its data base, is poised to be the next standard hip screening method. The first UK hands-free PennHIP course will take place in Cambridge on 3rd December 2009. Further information about PennHIP can be found at www.pennhip.org.
References:
-
Leighton EA, Linn JM, Willham RL, et al (1977): A genetic study of canine hip dysplasia. Am J Vet Res 38: 241-244
-
Hedhammer A, Olsson SE, Andersson SA, et al (1979): Canine hip dysplasia: Study of heritability in 401 litters of German shepherd dogs. JAVMA 174; 1012-1016
-
Reed AL, Keller GG, Vogt DW, et al (2000): Effect of dam and sire qualitative hip conformation on progeny hip conformation. JAVMA 217: 675-680
-
Falconer DS. Introduction to quantitative genetics. Ed 3. New York, Longman Scientific and Technical, 1989.
-
Smith GK, Mayhew PD, Kapatkin AS, et al (2001). Evaluation of risk factors for degenerative joint disease associated with hip dysplasia in German Shepherd dogs, Golden Retrievers, Labrador Retrievers and Rottweilers. JAVMA 219; 1719-1724
Further reading:
http://research.vet.upenn.edu/pennhip/ScienceandResearch/ScientificReports/tabid/3330/Default.aspx
Figure 1

PennHIP compression view
Figure 2

PennHIP distraction view
Figure 3
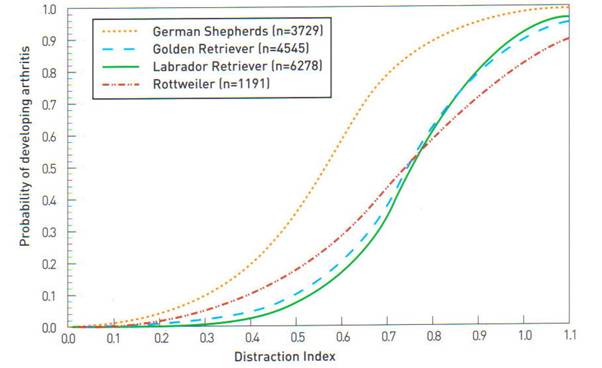
Figure 3
Depiction of the probability of developing osteoarthritis in 4 different breeds of dog at 24 months of age.